Anxiety vs Depression: A Reciprocal Relationship
Since Anxiety and depression appear to be associated with all mental disorders and since anxiety appears to be a key source of physiological distress and fatigue (Selye etc), the ISI was built to find relationships between anxiety and depression and key dimensions of psycho-social behavior. In other words what social behavior patterns might be most vulnerable to anxiety and depression. Since Toxic Stress is a key source of mental and psychological maladjustment and disease (Shonkoff & Garner, 2012), then it is likely that they will display key aberrations from the norm in terms of social behavior and provide us with stereotypical profiles. Given this information we may be able to specifically address individual weaknesses in these key areas to help encourage and support client behavior patterns that will likely reduce their levels of anxiety, depression and social distress. This approach is akin to the discovery by the Becks of the automatic thought and emotion patterns associated with depression, anxiety and mental disorder. The Diathesis Stress model predicts that these behaviors are both transgenerational and generic (RNA based) and classical and operantly transmitted in the family of origin.
To begin the analysis we need to investigate the relationship between anxiety and depression. Observations from the New Mind database suggest that anxiety emerges first and leads to depression and this model has strong support in the present research. The qEEG asymmetry suggests that as anxiety reaches significant levels with the appearance of increasing beta asymmetry, depressive symptoms begin to be reported by clients. At this point alpha asymmetries begin to progressively emerge and typically a mix of moderate levels of symptoms of anxiety and depression with correlating equal levels of alpha and beta asymmetries (Soutar, 2016). As severe depression symptoms along with total alpha asymmetry manifest beta migrates to the left hemisphere. This pattern should be reflected in the ISI measures of large sample groups.
Descriptive statistical analysis seems to support this perspective. Initially those with subclinical anxiety scores on the ISI (10-17) have corresponding subclinical depressions scores of 16 (N = 981). As anxiety moves into the low clinical range (18-20), depression score increase to low depression scores of 20 (18-20) (N = 160). As Anxiety moves into scores moderate range (21-25), depression scores move into moderate levels as well at 22 (N = 194) and the percent of the population inhabiting this range increases as well. As we move into high Anxiety scores (25-30) the depressions cores increase as well with a mean of 25 (N = 41). So the number of people of individuals drops off precipitously.
Inspecting this dynamic from the depression side we see a different picture. We see a similar pattern with subclinical depression showing very low anxiety scores of 11 (N = 1246), but low depression showing anxiety scores of 15 (N = 332). So anxiety is attenuated in the Depression Group whereas the anxiety moderate group was showing depression keeping pace. Moderate depression continues to show lower anxiety scores of 16 (331) than the depression scores of the anxiety group which also kept pace. Then finally at hi depression scores showing anxiety scores of 21 (N= 137) are showing moderate anxiety.
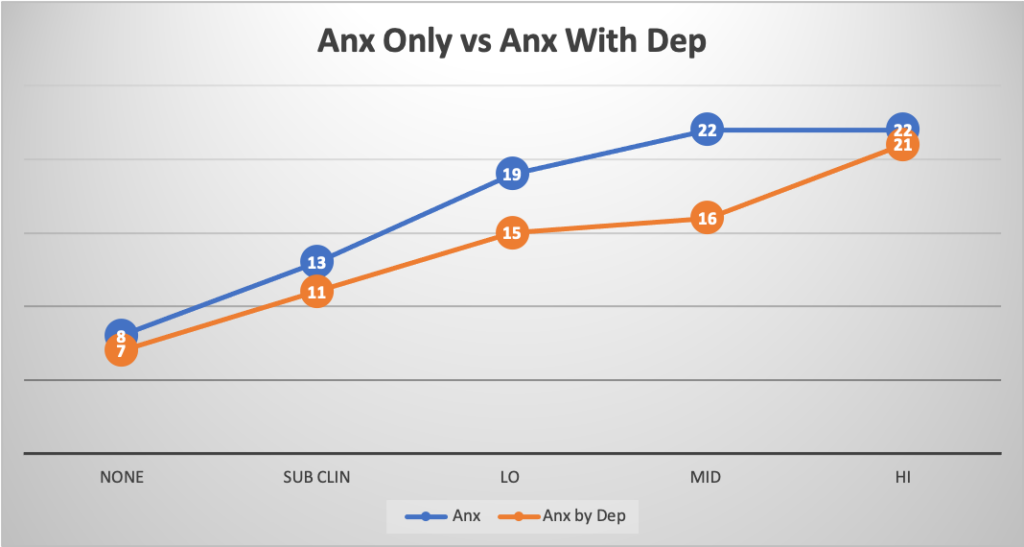
In the chart above ( N= 2393) the blue line shows mean anxiety scores of those reporting subclinical or no depression. The orange line show mean anxiety scores in those with depression as it increases. Note that the anxiety scores are lower in those with depression suggesting that depression modifies or reduces the experience of anxiety. Anxiety scores never reach above 25 without depression being present. In those with depression anxiety scores do reach as high as 30 and this group comprises only .01% of the entire sample, so it is very rare. 137 individuals reach levels of hi depression in this group which is .06% and so significantly greater.
This suggests that as anxiety emerges, depression keeps pace but at the high anxiety levels the number of individuals falls off and we see more depressive subjects. Of special interest is that as depression increases anxiety lags behind.
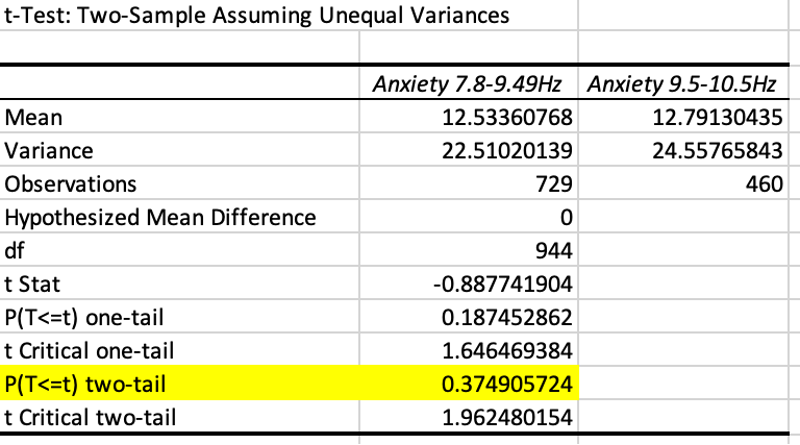
Anxiety is not greater in low frequency than normal frequency alpha (Cz). This is likely due to the muting effects of depression on amygdala input as alpha asymmetry increases.
Subclinical depression subjects display very low anxiety scores suggesting that these are passing episodes of negative mood related to daily challenges. These clients are reacting to typical social stressors experienced by most people in the population on a regular basis. Subclinical anxiety has fewer depressives than those with subclinical depression have anxiety (981 vs 1246). This would be expected if anxiety typically precedes depression as proposed by the physiological research to date (Wang & Michaelis, 2011). Individuals are concerned about their social performance but have not succumbed to serious doubts about their self-efficacy. They are getting sufficient rest, recreation and sleep to clear the glutamate and other necrotic debris from their neuronal interstitial regions.
The correlation between anxiety and inhibited was conducted on N = 2392 and as expected the correlation was very high at .62 or 62%. Anxiety had a low correlation however with impulsivity at .23, which we expected from clinical observation would be higher. So other factors are influencing impulsivity as well anxiety and likely those factors may be found in frontal levels of theta which are statistically associated with anxiety noted later in the analysis.
Impulse control was frequently observed to be elevated in individuals with anxiety but the correlation was low around .26. Looking at other contributing factors we ran correlations and regression analysis on impulsivity by anxiety and perfectionism but still found very low correlations and r squared values. Considering the possibility that depression could reduce impulsivity as seen in many TOVA tests, those who had depression in addition to anxiety were removed to provide a pure anxiety group. This still showed no significance. Finally we also filtered anxiety additionally into a high and low perfectionism group Perfectionism < ISI score of 12. These two groups were compared with a t-test. Those with pure anxiety who had perfectionism high scored significantly higher on impulsivity than those who had perfectionism low. Apparently perfectionism plays a part in impulsivity as well.
| t-Test: Two-Sample Assuming Unequal Variances |
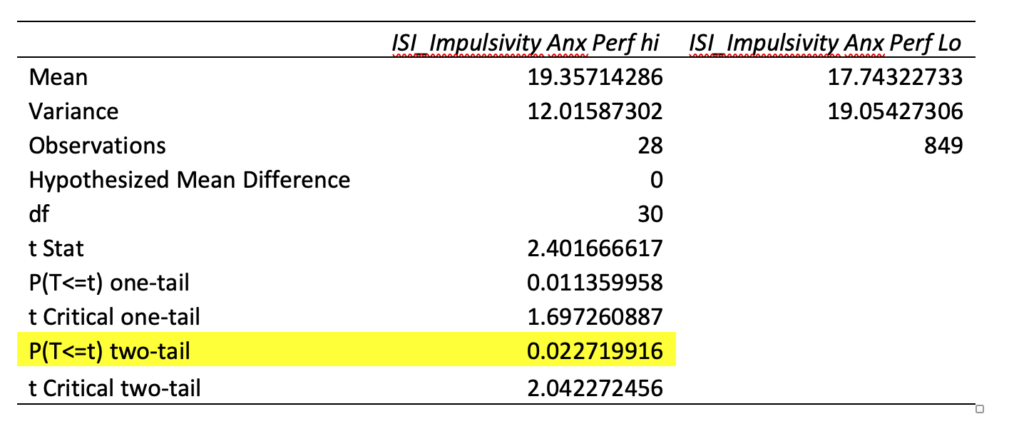
So in summary individuals with anxiety and or depression have higher levels of socially inhibited behavior. Those with anxiety only as well as a high level of perfectionism tended to be more impulsive than those with low perfectionism.
At the New Mind clinic, as well as other clinics we conferred with, we began to observe consistently high scores in the dimension of perfectionism in those who scored high in anxiety and high scores in competitiveness and perfectionism combined arising at the same time we noticed elevated scores in depression. It made sense to us that clients who were anxious might try harder to control their environments and ensure greater stability, predictability and controllability and personal safety. We see extreme versions of this in OCD with compulsive checking, cleaning, and other ritual behaviors. To confirm this observation we looked at different levels of anxiety in the ISI and what their associated scores were with respect to Perfectionism.
Peak Performers display a Perfectionism mean score of 16. Those with high anxiety score in the 25-30 range (N = 42) showed a perfectionism mean score of 18. This group has a small N size because most individual appear to shift into depression once anxiety approaches a score 25 (more on this later). Mid-level anxiety scores (20-25) tend to average around 16 (N = 195) on Perfectionism and low anxiety (15-20) tend to score in the 16 range on Perfectionism as well (N = 160). Those with no anxiety (6-10) tend to have mean scores of 15, lower than Peak Performers. Unlike the clinical sample whose anxiety is usually in the mid-range when they score 16 on perfectionism, the Peak Performers all scored below 10. Speculation: This may be because their perfectionism is not a function of their anxiety level and that they channel any anxiety constructively into actions that reduce their fears and concerns and they have more of a sense of empowerment/self-efficacy and a more internal locus of control.
Because few people reach scores higher than 25 on anxiety, in this national sample 42 out of 2393 or .01%, and the majority develop co-existing depression, 784 out of 2393 or 30% (which is consistent with the reported national incidence and cross validate the quality of our sample), it is likely that the majority of people with high anxiety become significantly depressed and that it appears to blunt the symptoms of anxiety and reduce their self-report of depression. This is consistent with the physiology of anxiety and depression. Excessive excitotoxicity from fear and anxiety increases glutamate levels and sleep deprivation from anxiety reduces opportunities to clear the excess glutamate during rest (Moritani, 2005). This in turn elicits a pro-inflammatory response in the brain which re- routes 5HTP from serotonin production into quinolinic acid production, thus reducing serotonin effects (Wang & Michaelis, 2010) and resulting in depression. In this sense, physiologically depression is a consequence of chronic anxiety and likely a protective response rather than a mysterious bad thing that happens out of the blue requiring immediate medication. As we shall see, as depression increases , anxiety decreases, supporting the protective hypothesis.
It makes sense then to investigate the impact of anxiety on competitiveness, as it likely contributes as well.
Moritani, T., Smoker, W. R. K., Sato, Y., Numaguchi, Y., Westesson, P. A. (2005). Diffusion-weighted imaging of acute excitotoxic brain injury. AJNR Am J Neuroradiol 26:216–228.
Shonkoff, J. & Garner, A. (2012). The lifelong effects of childhood adversity and toxic stress. Pediatrics,129, 1, e32-e46.
Wang, X., Michaelis, E. K. (2010). Selective neuronal vulnerability to oxidative stress in the brain. Frontiers in Aging Neuroscience. Volume 2, Article 12, 1-13.